




Verdens sykeste lidelser
«Tremannen» er ikke den eneste som har en gripende historie og lidelse.
(SIDE2): Ekstreme og sjeldne lidelser har gjort et knippe mennesker kjente opp gjennom tidene. Mange har fått hjelp etter mye medieomtale, og flere av personene sier de lever et normalt liv, på tross av sin besynderlige sykdom. Her er noen av de mest kjente og uvanlige lidelsene:
«ULVEMANNEN»: Fajardo Aceves Jesus Manuel fra Mexico er kjent som «Ulvemannen» på grunn av sin ekstreme hårvekst. Tilstanden er et resultat av «hiper tricosis», en sykdom som fører til overflod av hår. Fajardo Aceves Jesus Manuel mener han har arvet lidelsen etter sin oldemor. Foruten at han ser annerledes ut, hevder han at han lever et helt normalt liv.
«TREMANNEN»: Indonesiske Dede lider av en sykdom der store deler av kroppen hans er dekket av barkeliknende vorter. Hudspesialist tror det kan være en kombinasjon av viruset som forårsaker vorter og en genetisk sykdom som gjør at immunforsvaret hans svekkes. Les mer om historien til Dede her.
«HORNMANNEN»: Opp fra bakhodet til kinesiske Ma Zhong Nan stikker det opp et ti centimeter langt horn. Det begynte å vokse for om lag fem år siden, etter at han fikk et lite kutt mens han kjemmet håret. Les mer om hornmannen her.
TRICHOPHAGIA: Lidelsen er meget sjelden og innebærer at vedkommende spiser på sitt eget hår. Dette kan gi store hårballer i magesekken. Les mer hos Wikipedia.
En 18 år gammel kvinne som gjennom hele livet hadde hatt god helse opplevde plutselig ubehag. Etter fem måneder med magesmerter, kvalme, hevelser og vekttap oppsøkte hun eksperter. Da legene undersøkte kvinnens mage fant de utrolig nok en hårball på 4,5 kilo. Les saken her: Fant kjempehårball i kvinnemage
EKSTREM OVERVEKT: Meksikanske Manuel Uribe veide 556 kilo i september i fjor. På grunn av sin høye vekt hadde han ikke kunnet forlate sengen på fem år. I sommer var det første gang Uribe var utendørs på lang tid. Han kunne endelig forlate rommet sitt etter å ha fullført en streng diett. Les mer: Redd verdens feteste
MIKROSKOPISKE KRANIER :
Microcephaly er en nervelidelse hvor omkretsen av hodet er betydelig mye mindre enn normalt for en persons alder og kjønn. Lidelsen kan være medfødt eller utvikle seg i de første leveårene. Den kommer av ulike tilstander som medfører anormal vekst av hjernen eller fra syndromer som assosieres med kromosom abnormitet.
Zip og pip eller Jennie Lee og Elvira Snow som de egentlig het ble kalt for «The Snow Twins». De led av microcephaly og var som de fleste som lider av dette syndromet mentalt tilbakestående. De reiste sammen med World Circus Sideshow i første halvdel av 1900-tallet sammen med mange andre mennesker som hadde unormale lidelser, men hadde tilholdssted på Coney Island.
«ARMLESS WONDER»: Martha Morris ble født tidlig på 1900-tallet i Chicago. Hun manglet begge armene, og deler av beina. Kvinnen, som fikk navnet «Armless Wonder», var ikke i stand til å kle på seg selv eller gå. Hun kom seg rundt ved hjelp av at folk trillet henne i en rullestol. Hun ble kjent for å holde ulike utstillinger. Da demonstrerte Morris imponerende ferdigheter ved å skrive med tærne som om det skulle vært fullt utviklet fingre.
Histopathology Brain– Alzheimer disease
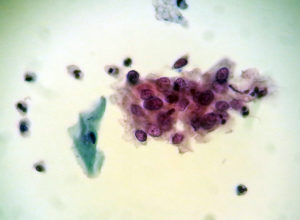 Gruppe med maligne celler.
Gruppe med maligne celler.
Sykdom. PDF.
Vitenskap, kultur eller begrep for sårbarhet, håp, mestring og mot?
Bjørn Hofmann, Høgskolen i Gjøvik, Universitetet i Oslo.
History of Morgellons disease: from delusion to definition. PDF.
(Er dette en “ekte” sykdom? Ingen patologer har vel sett dette? Har noen denne i Norge?)


Fra Folkehelseinstituttet:
Hva er sesonginfluensa?
Hvert år i perioden desember til april rammes befolkningen på den nordlige halvkule av influensaepidemier. Dette kalles sesonginfluensa. To typer av influensavirus, type A og B, er årsak til disse epidemiene. Fra år til år utvikler hvert av influensavirusene nye varianter som gjør vår immunitet mot de gamle variantene utdatert.
Influensapandemier i historien
Epidemier som ser ut til å ha vært influensa, er kjent langt tilbake i tid. Det er særlig de ekstraordinært store epidemiene som har blitt nedtegnet. Til sammen 19 slike svære influensaepidemier er kjent fra historien. Vi kaller dem influensapandemier. Bare influensa A kan gi en pandemi.
Den første pandemien ble beskrevet i 1580. Den største var Spanskesyken i 1918-19, som førte til 25-40 millioner dødsfall i verden. I Norge døde cirka 15 000 personer.
De tre siste større pandemiene var:
- Asiasyken i 1957
- Hong Kong-syken i 1968
- H1N1-pandemien i 2009/2010 (svineinfluensa)
Varianten av A(H1N1)-virus som førte til pandemien i 2009/2010, kalles ofte svineinfluensa siden de nærmeste slektningene vi kjenner er svineinfluensavirus. Varianten utgjør i dag ett av de vanlige sesonginfluensavirusene og har siden pandemien blitt kalt A(H1N1)pdm09.
Forekomst av sesonginfluensa
Andelen som blir syke med influensa varierer fra sesong til sesong, avhengig av immuniteten i befolkningen mot sirkulerende virus, vaksinasjonsdekning og de sykdomsfremkallende egenskaper til selve viruset. I år med større epidemier kan 10-30 prosent av den norske befolkningen bli smittet. I en gjennomsnittlig sesong vil 5-10% av alle voksne og 20-30% av alle barn bli smittet.
Tidspunktet for influensautbruddene er illustrert ved kurven under. Den viser at influensautbruddene vanligvis starter rundt jul/nyttår, og varer i omtrent 12 uker. Influensatoppen har de siste sesongene falt enten rundt nyttår eller omkring vinterferien. Dette kan imidlertid variere mellom sesonger.

Estimater basert på data fra perioden 1975-2004 tyder på at omtrent 900 dødsfall i året kan knyttes til influensa i Norge. Dette er imidlertid et gjennomsnitt og kan variere mye fra år til år. Det er alt overveiende eldre og personer med alvorlig bakenforliggende sykdom som dør som følge influensa.
Fakta om koronavirus (coronavirus)
Publisert Oppdatert
Det nye koronaviruset ble oppdaget i januar 2020 og ny kunnskap tilkommer stadig. Hva vet vi om utbruddet, viruset, sykdommen og risiko? Informasjon og råd vil bli justert og oppdatert i henhold til utbruddets utvikling og kunnskap om infeksjonen.

Om utbruddet
Et tidligere ukjent koronavirus har forårsaket et pågående utbrudd av luftveisinfeksjon. Utbruddet startet i storbyen Wuhan i Hubei-provinsen i Kina i desember 2019, og viruset ble identifisert av kinesiske helsemyndigheter 7. januar 2020.
Det nye viruset er et koronavirus (coronavirus) og har etterhvert fått navnet SARS-CoV-2 som kan gi luftveisinfeksjon hos mennesker. I mange tilfeller har det kun gitt mild sykdom, men det rapporteres også om tilfeller av alvorlig sykdom og dødsfall.
Utbruddet startet i millionbyen Wuhan i Hubei-provinsen sentralt i Kina. Smitten ble i begynnelsen knyttet til et stort matmarked i byen, Huanan Seafood Wholesale Market, med sjømat og ulike typer levende dyr, noe som kan tyde på at smitten opprinnelig kommer fra dyr.
Sykdommen smitter mellom mennesker og det er sett smitte til helsepersonell og andre nærkontakter. Det rapporteres stadig flere tilfeller fra andre kinesiske områder og andre land, også i Europa.
For oppdatert informasjon om utbruddet i Europa og hele verden:
- Det europeiske smittevernbyråets (ECDCs) nettsider om koronavirusutbruddet
- Verdens helseorganisasjons (WHOs) nettside om koronavirusutbruddet
30. januar 2020 erklærte WHO utbruddet som en “alvorlig hendelse av betydning for internasjonal folkehelse”. Erklæringen er ment å styrke Verdens helseorganisasjon (WHO) sin koordinering av innsatsen mot videre spredning av sykdom forårsaket av det nye viruset.
Om viruset
Det nye koronaviruset er et tidligere ukjent virus, men har visse genetiske likheter med SARS-viruset (Severe Acute Respiratory Syndrome) som også tilhører koronavirusfamilien. Viruset som forårsaker MERS (Middle East Respiratory Syndrome) er et annet koronavirus.
Man antar at smittemåten er dråpe- og kontaktsmitte som for andre koronavirus.
Koronavirusfamilien omfatter mange ulike virus som kan gi luftveisinfeksjon. Mange koronavirus gir bare forkjølelse, mens andre kan gi mer alvorlig sykdom og i noen tilfeller forårsake dødsfall. Koronavirus finnes også hos dyr. I sjeldne tilfeller kan slike koronavirus utvikle seg slik at de kan smitte fra dyr til mennesker og mellom mennesker, slik man så under SARS-epidemien i 2002. Da kom smitten antagelig fra flaggermus via sivettkatter og andre dyr. Dromedarer og kameler er smittekilde for sykdommen MERS som ble oppdaget i 2012.
From Biopsy to Diagnosis: How Pathologists Diagnose Cancer and Other Diseases.
This video provides a glimpse into the world of pathology by showing how pathologists and other laboratory professionals help to diagnose patients’ biopsies. This behind-the-scenes look into the University of Michigan Department of Pathology shows how tissue is prepared to be viewed under a microscope and what pathologists are looking for in order to determine a diagnosis.
Mammografiscreening er kontroversielt!
Mange mener det er viktig å finne små svulster så tidlig som mulig, og behandle disse for å få god overlevelse. Imidlertid oppstår det sannsynlig flere ganger naturlig små svulster som imidlertid forsvinner “naturlig” i kroppen, og også i bryst. En mulig årsak til dette kan bl.a.henge sammen med autofagi (selv-spising) som er sentralt i kroppens eget forsvarsystem for å bekjempe visse sykdommer. Se også Nobelprisen i medisin 2016 til japaneren Yoshinori Ohsumi.
Med mammografiscreening får man også en del uheldige sideefekter som bl. a. overbehandling og pasientfeil.
Mange mener det hjelper i forhold til overlevelse, selv om bildet trolig er noe anderledes:
Dr. László Tabár is synonymous with innovation and mammography.
László Tabár, M.D., F.A.C.R. (Hon) har nok bidrad sterkt til den svært positive tankegang om at man bør innføre mammografiscreening! Se hans hjemmesider som er “Big business“.
Statestics: Dessverre Mye error/ biasfeil!
“The average human being has 1 breast and 1 testicle”- (Des McHale)”.
Introduction
According to the World Health Organization (WHO), viral diseases continue to emerge and represent a serious issue to public health. In the last twenty years, several viral epidemics such as the severe acute respiratory syndrome coronavirus (SARS-CoV) in 2002 to 2003, and H1N1 influenza in 2009, have been recorded. Most recently, the Middle East respiratory syndrome coronavirus (MERS-CoV) was first identified in Saudi Arabia in 2012.
In a timeline that reaches the present day, an epidemic of cases with unexplained low respiratory infections detected in Wuhan, the largest metropolitan area in China’s Hubei province, was first reported to the WHO Country Office in China, on December 31, 2019. Published literature can trace the beginning of symptomatic individuals back to the beginning of December 2019. As they were unable to identify the causative agent, these first cases were classified as “pneumonia of unknown etiology.” The Chinese Center for Disease Control and Prevention (CDC) and local CDCs organized an intensive outbreak investigation program. The etiology of this illness is now attributed to a novel virus belonging to the coronavirus (CoV) family, COVID-19.
On February 11, 2020, the WHO Director-General, Dr. Tedros Adhanom Ghebreyesus, announced that the disease caused by this new CoV was a “COVID-19,” which is the acronym of “coronavirus disease 2019”. In the past twenty years, two additional coronavirus epidemics have occurred. SARS-CoV provoked a large-scale epidemic beginning in China and involving two dozen countries with approximately 8000 cases and 800 deaths, and the MERS-CoV that began in Saudi Arabia and has approximately 2,500 cases and 800 deaths and still causes as sporadic cases.
This new virus seems to be very contagious and has quickly spread globally. In a meeting on January 30, 2020, per the International Health Regulations (IHR, 2005), the outbreak was declared by the WHO a Public Health Emergency of International Concern (PHEIC) as it had spread to 18 countries with four countries reporting human-to-human transmission. An additional landmark occurred on February 26, 2020, as the first case of the disease, not imported from China, was recorded in the United States.
Initially, the new virus was called 2019-nCoV. Subsequently, the task of experts of the International Committee on Taxonomy of Viruses (ICTV) termed it the SARS-CoV-2 virus as it is very similar to the one that caused the SARS outbreak (SARS-CoVs).
The CoVs have become the major pathogens of emerging respiratory disease outbreaks. They are a large family of single-stranded RNA viruses (+ssRNA) that can be isolated in different animal species.[1] For reasons yet to be explained, these viruses can cross species barriers and can cause, in humans, illness ranging from the common cold to more severe diseases such as MERS and SARS. Interestingly, these latter viruses have probably originated from bats and then moving into other mammalian hosts — the Himalayan palm civet for SARS-CoV, and the dromedary camel for MERS-CoV — before jumping to humans. The dynamics of SARS-Cov-2 are currently unknown, but there is speculation that it also has an animal origin.
The potential for these viruses to grow to become a pandemic worldwide seems to be a serious public health risk. Concerning COVID-19, the WHO raised the threat to the CoV epidemic to the “very high” level, on February 28, 2020. Probably, the effects of the epidemic caused by the new CoV has yet to emerge as the situation is quickly evolving. World governments are at work to establish countermeasures to stem possible devastating effects. Health organizations coordinate information flows and issues directives and guidelines to best mitigate the impact of the threat. At the same time, scientists around the world work tirelessly, and information about the transmission mechanisms, the clinical spectrum of disease, new diagnostics, and prevention and therapeutic strategies are rapidly developing. Many uncertainties remain with regard to both the virus-host interaction and the evolution of the epidemic, with specific reference to the times when the epidemic will reach its peak.
At the moment, the therapeutic strategies to deal with the infection are only supportive, and prevention aimed at reducing transmission in the community is our best weapon. Aggressive isolation measures in China have led to a progressive reduction of cases in the last few days. In Italy, in geographic regions of the north of the peninsula, political and health authorities are making incredible efforts to contain a shock wave that is severely testing the health system.
In the midst of the crisis, the authors have chosen to use the “Statpearls” platform because, within the PubMed scenario, it represents a unique tool that may allow them to make updates in real-time. The aim, therefore, is to collect information and scientific evidence and to provide an overview of the topic that will be continuously updated.
Etiology
CoVs are positive-stranded RNA viruses with a crown-like appearance under an electron microscope (coronamis the Latin term for crown) due to the presence of spike glycoproteins on the envelope. The subfamilyOrthocoronavirinaeof theCoronaviridaefamily (orderNidovirales) classifies into four genera of CoVs: Alphacoronavirus (alphaCoV), Betacoronavirus (betaCoV), Deltacoronavirus (deltaCoV), and Gammacoronavirus (gammaCoV). Furthermore, the betaCoV genus divides into five sub-genera or lineages.[2] Genomic characterization has shown that probably bats and rodents are the gene sources of alphaCoVs and betaCoVs. On the contrary, avian species seem to represent the gene sources of deltaCoVs and gammaCoVs.
Members of this large family of viruses can cause respiratory, enteric, hepatic, and neurological diseases in different animal species, including camels, cattle, cats, and bats. To date, seven human CoVs (HCoVs) — capable of infecting humans — have been identified. Some of HCoVs were identified in the mid-1960s, while others were only detected in the new millennium.
In general, estimates suggest that 2% of the population are healthy carriers of a CoV and that these viruses are responsible for about 5% to 10% of acute respiratory infections.[3]
-
Common human CoVs: HCoV-OC43, and HCoV-HKU1 (betaCoVs of the A lineage); HCoV-229E, and HCoV-NL63 (alphaCoVs). They can cause common colds and self-limiting upper respiratory infections in immunocompetent individuals. In immunocompromised subjects and the elderly, lower respiratory tract infections can occur.
-
Other human CoVs: SARS-CoV, SARS-CoV-2, and MERS-CoV (betaCoVs of the B and C lineage, respectively). These cause epidemics with variable clinical severity featuring respiratory and extra-respiratory manifestations. Concerning SARS-CoV, MERS-CoV, the mortality rates are up to 10% and 35%, respectively.
Thus, SARS-CoV-2 belongs to the betaCoVs category. It has round or elliptic and often pleomorphic form, and a diameter of approximately 60–140 nm. Like other CoVs, it is sensitive to ultraviolet rays and heat. Furthermore, these viruses can be effectively inactivated by lipid solvents including ether (75%), ethanol, chlorine-containing disinfectant, peroxyacetic acid and chloroform except for chlorhexidine.
In genetic terms, Chan et al. have proven that the genome of the new HCoV, isolated from a cluster-patient with atypical pneumonia after visiting Wuhan, had 89% nucleotide identity with bat SARS-like-CoVZXC21 and 82% with that of human SARS-CoV[4]. For this reason, the new virus was called SARS-CoV-2. Its single-stranded RNA genome contains 29891 nucleotides, encoding for 9860 amino acids. Although its origins are not entirely understood, these genomic analyses suggest that SARS-CoV-2 probably evolved from a strain found in bats. The potential amplifying mammalian host, intermediate between bats and humans, is, however, not known. Since the mutation in the original strain could have directly triggered virulence towards humans, it is not certain that this intermediary exists.
Transmission
Because the first cases of the CoVID-19 disease were linked to direct exposure to the Huanan Seafood Wholesale Market of Wuhan, the animal-to-human transmission was presumed as the main mechanism. Nevertheless, subsequent cases were not associated with this exposure mechanism. Therefore, it was concluded that the virus could also be transmitted from human-to-human, and symptomatic people are the most frequent source of COVID-19 spread. The possibility of transmission before symptoms develop seems to be infrequent, although it cannot be excluded. Moreover, there are suggestions that individuals who remain asymptomatic could transmit the virus. This data suggests that the use of isolation is the best way to contain this epidemic.
As with other respiratory pathogens, including flu and rhinovirus, the transmission is believed to occur through respiratory droplets from coughing and sneezing. Aerosol transmission is also possible in case of protracted exposure to elevated aerosol concentrations in closed spaces. Analysis of data related to the spread of SARS-CoV-2 in China seems to indicate that close contact between individuals is necessary. The spread, in fact, is primarily limited to family members, healthcare professionals, and other close contacts.
Based on data from the first cases in Wuhan and investigations conducted by the China CDC and local CDCs, the incubation time could be generally within 3 to 7 days and up to 2 weeks as the longest time from infection to symptoms was 12.5 days (95% CI, 9.2 to 18).[5] This data also showed that this novel epidemic doubled about every seven days, whereas the basic reproduction number (R0 – R naught) is 2.2. In other words, on average, each patient transmits the infection to an additional 2.2 individuals. Of note, estimations of the R0 of the SARS-CoV epidemic in 2002-2003 were approximately 3.[6]
It must be emphasized that this information is the result of the first reports. Thus, further studies are needed to understand the mechanisms of transmission, the incubation times and the clinical course, and the duration of infectivity.
Epidemiology
Data provided by the WHO Health Emergency Dashboard (March 03, 10.00 am CET) report 87,137 confirmed cases worldwide since the beginning of the epidemic. Of these, 2977 (3.42%) have been fatal. About 92% (79,968) of the confirmed cases were recorded in China, where almost all the deaths were also recorded (2,873, 96.5%). Of note, the “confirmed” cases reported between February 13, 2020, and February 19, 2020, include both laboratory-confirmed and clinically diagnosed patients from the Hubei province.
Outside China, there are 7169 confirmed cases in 59 countries including the Republic of Korea (3736 cases), Italy (1128), international conveyance (Diamond Princess, 705 cases), the Islamic Republic of Iran (593), Japan (239), Singapore (102), France (100), United States of America (62), Germany (57), Kuwait (45), Spain (45), Thailand (42), Bahrain (40), Australia (25), Malaysia (24), United Kingdom (23), Canada (19), United Arab Emirates (19), Switzerland (18), Viet Nam (16), Norway (15), Iraq (13), Sweden (13), Austria (10), Croatia (7), Israel (7), Netherlands (7), Oman (6), Pakistan (4), Azerbaijan (3), Denmark (3), Georgia (3), Greece (3), India (3), Philippines (3), Romania (3). Moreover, two cases were recorded respectively in Brazil, Finland, Lebanon, Mexico, the Russian Federation, and a single case each in Afghanistan, Algeria, Belarus, Belgium, Cambodia, Ecuador, Egypt, Estonia, Ireland, Lithuania, Monaco, Nepal, New Zealand, Nigeria, North Macedonia, Qatar, San Marino, and Sri Lanka.
The most up-to-date source for the epidemiology of this emerging pandemic can be found at the following sources:
-
The WHO Novel Coronavirus (COVID-19) Situation Board
-
The Johns Hopkins Center for Systems Science and Engineering site for Coronavirus Global Cases COVID-19, which uses openly public sources to track the spread of the epidemic.
Pathophysiology
CoVs are enveloped, positive-stranded RNA viruses with nucleocapsid. For addressing pathogenetic mechanisms of SARS-CoV-2, its viral structure, and genome must be considerations. In CoVs, the genomic structure is organized in a +ssRNA of approximately 30 kb in length — the largest known RNA viruses — and with a 5′-cap structure and 3′-poly-A tail. Starting from the viral RNA, the synthesis of polyprotein 1a/1ab (pp1a/pp1ab) in the host is realized. The transcription works through the replication-transcription complex (RCT) organized in double-membrane vesicles and via the synthesis of subgenomic RNAs (sgRNAs) sequences. Of note, transcription termination occurs at transcription regulatory sequences, located between the so-called open reading frames (ORFs) that work as templates for the production of subgenomic mRNAs. In the atypical CoV genome, at least six ORFs can be present. Among these, a frameshift between ORF1a and ORF1b guides the production of both pp1a and pp1ab polypeptides that are processed by virally encoded chymotrypsin-like protease (3CLpro) or main protease (Mpro), as well as one or two papain-like proteases for producing 16 non-structural proteins (nsps). Apart from ORF1a and ORF1b, other ORFs encode for structural proteins, including spike, membrane, envelope, and nucleocapsid proteins.[1] and accessory proteic chains. Different CoVs present special structural and accessory proteins translated by dedicated sgRNAs.
Pathophysiology and virulence mechanisms of CoVs, and therefore also of SARS-CoV-2 have links to the function of the nsps and structural proteins. For instance, research underlined that nsp is able to block the host innate immune response.[7] Among functions of structural proteins, the envelope has a crucial role in virus pathogenicity as it promotes viral assembly and release. However, many of these features (e.g., those of nsp 2, and 11) have not yet been described.
Among the structural elements of CoVs, there are the spike glycoproteins composed of two subunits (S1 and S2). Homotrimers of S proteins compose the spikes on the viral surface, guiding the link to host receptors.[8]Of note, in SARS-CoV-2, the S2 subunit — containing a fusion peptide, a transmembrane domain, and cytoplasmic domain — is highly conserved. Thus, it could be a target for antiviral (anti-S2) compounds. On the contrary, the spike receptor-binding domain presents only a 40% amino acid identity with other SARS-CoVs. Other structural elements on which research must necessarily focus are the ORF3b that has no homology with that of SARS-CoVs and a secreted protein (encoded by ORF8), which is structurally different from those of SARS-CoV.
In international gene banks such as GenBank, researchers have published several Sars-CoV-2 gene sequences. This gene mapping is of fundamental importance allowing researchers to trace the phylogenetic tree of the virus and, above all, the recognition of strains that differ according to the mutations. According to recent research, a spike mutation, which probably occurred in late November 2019, triggered jumping to humans. In particular, Angeletti et al. compared the Sars-Cov-2 gene sequence with that of Sars-CoV. They analyzed the transmembrane helical segments in the ORF1ab encoded 2 (nsp2) and nsp3 and found that position 723 presents a serine instead of a glycine residue, while the position 1010 is occupied by proline instead of isoleucine.[9]The matter of viral mutations is key for explaining potential disease relapses.
Research will be needed to determine the structural characteristics of SARS-COV-2 that underlie the pathogenetic mechanisms. Compared to SARS, for example, initial clinical data show less extra respiratory involvement, although due to the lack of extensive data, it is not possible to draw definitive clinical information.
Histopathology
Tian et al.[10]and others reported histopathological data obtained on the lungs of two patients who underwent lung lobectomies for adenocarcinoma and retrospectively found to have had the infection at the time of surgery. Apart from the tumors, the lungs of both ‘accidental’ cases showed edema and important proteinaceous exudates as large protein globules. The authors also reported vascular congestion combined with inflammatory clusters of fibrinoid material and multinucleated giant cells and hyperplasia of pneumocytes.
History and Physical
The clinical spectrum of COVID-19 varies from asymptomatic or paucisymptomatic forms to clinical conditions characterized by respiratory failure that necessitates mechanical ventilation and support in an intensive care unit (ICU), to multiorgan and systemic manifestations in terms of sepsis, septic shock, and multiple organ dysfunction syndromes (MODS). In one of the first reports on the disease, Huang et al. illustrated that patients (n. 41) suffered from fever, malaise, dry cough, and dyspnea. Chest computerized tomography (CT) scans showed pneumonia with abnormal findings in all cases. About a third of those (13, 32%) required ICU care, and there were 6 (15%) fatal cases.[11]
The case studies of Li et al. published in the New England Journal of Medicine (NEJM) on January 29, 2020, encapsulates the first 425 cases recorded in Wuhan.[5] Data indicate that the patients’ median age was 59 years, with a range of 15 to 89 years. Thus, they reported no clinical cases in children below 15 years of age. There were no significant gender differences (56% male). Clinical and epidemiological data from the Chinese CDC and regarding 72,314 case records (confirmed, suspected, diagnosed, and asymptomatic cases) were shared in the Journal of the American Medical Association (JAMA) (February 24, 2020), providing an important illustration of the epidemiologic curve of the Chinese outbreak.[12] There were 62% confirmed cases, including 1% of cases that were asymptomatic, but were laboratory-positive (viral nucleic acid test). Furthermore, the overall case-fatality rate (on confirmed cases) was 2.3%. Of note, the fatal cases were primarily elderly patients, in particular those aged ≥ 80 years (about 15%), and 70 to 79 years (8.0%). Approximately half (49.0%) of the critical patients and affected by preexisting comorbidities such as cardiovascular disease, diabetes, chronic respiratory disease, and oncological diseases, died. While 1% of patients were aged 9 years or younger, no fatal cases occurred in this group.
The authors of the Chinese CDC report divided the clinical manifestations of the disease by there severity:
-
Mild disease: non-pneumonia and mild pneumonia; this occurred in 81% of cases.
-
Severe disease: dyspnea, respiratory frequency ≥ 30/min, blood oxygen saturation (SpO2) ≤ 93%, PaO2/FiO2 ratio [the ratio between the blood pressure of the oxygen (partial pressure of oxygen, PaO2) and the percentage of oxygen supplied (fraction of inspired oxygen, FiO2)] < 300, and/or lung infiltrates > 50% within 24 to 48 hours; this occurred in 14% of cases.
-
Critical disease: respiratory failure, septic shock, and/or multiple organ dysfunction (MOD) or failure (MOF); this occurred in 5% of cases.[12]
Data obtainable from reports and directives provided by health policy agencies, allow dividing the clinical manifestations of the disease according to the severity of the clinical pictures. The COVID-19 may present with mild, moderate, or severe illness. Among the severe clinical manifestations, there are severe pneumonia, ARDS, sepsis, and septic shock. The clinical course of the disease seems to predict a favorable trend in the majority of patients. In a percentage still to be defined of cases, after about a week there is a sudden worsening of clinical conditions with rapidly worsening respiratory failure and MOD/MOF. As a reference, the criteria of the severity of respiratory insufficiency and the diagnostic criteria of sepsis and septic shock can be used.[13]
Uncomplicated (mild) Illness
These patients usually present with symptoms of an upper respiratory tract viral infection, including mild fever, cough (dry), sore throat, nasal congestion, malaise, headache, muscle pain, or malaise. Signs and symptoms of a more serious disease, such as dyspnea, are not present. Compared to previous HCoV infections, non-respiratory symptoms such as diarrhea are challenging to find.
Moderate Pneumonia
Respiratory symptoms such as cough and shortness of breath (or tachypnea in children) are present without signs of severe pneumonia.
Severe Pneumonia
Fever is associated with severe dyspnea, respiratory distress, tachypnea (> 30 breaths/min), and hypoxia (SpO2 < 90% on room air). However, the fever symptom must be interpreted carefully as even in severe forms of the disease, it can be moderate or even absent. Cyanosis can occur in children. In this definition, the diagnosis is clinical, and radiologic imaging is used for excluding complications.
Acute Respiratory Distress Syndrome (ARDS)
The diagnosis requires clinical and ventilatory criteria. This syndrome is suggestive of a serious new-onset respiratory failure or for worsening of an already identified respiratory picture. Different forms of ARDS are distinguished based on the degree of hypoxia. The reference parameter is the PaO2/FiO2:
-
Mild ARDS: 200 mmHg < PaO2/FiO2 ≤ 300 mmHg. In not-ventilated patients or in those managed through non-invasive ventilation (NIV) by using positive end-expiratorypressure (PEEP) or a continuous positive airway pressure (CPAP) ≥ 5 cmH2O.
-
Moderate ARDS: 100 mmHg < PaO2/FiO2 ≤ 200 mmHg.
-
Severe ARDS: PaO2/FiO2 ≤ 100 mmHg.
When PaO2 is not available, a ratio SpO2/FiO2 ≤ 315 is suggestive of ARDS.
Chest imaging utilized includes chest radiograph, CT scan, or lung ultrasound demonstrating bilateral opacities (lung infiltrates > 50%), not fully explained by effusions, lobar, or lung collapse. Although in some cases, the clinical scenario and ventilator data could be suggestive for pulmonary edema, the primary respiratory origin of the edema is proven after the exclusion of cardiac failure or other causes such as fluid overload. Echocardiography can be helpful for this purpose.
Sepsis
According to the International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3), sepsis represents a life-threatening organ dysfunction caused by a dysregulated host response to suspected or proven infection, with organ dysfunction.[14] The clinical pictures of patients with COVID-19 and with sepsis are particularly serious, characterized by a wide range of signs and symptoms of multiorgan involvement. These signs and symptoms include respiratory manifestations such as severe dyspnea and hypoxemia, renal impairment with reduced urine output, tachycardia, altered mental status, and functional alterations of organs expressed as laboratory data of hyperbilirubinemia, acidosis, high lactate, coagulopathy, and thrombocytopenia. The reference for the evaluation of multiorgan damage and the related prognostic significance is the Sequential Organ Failure Assessment (SOFA) score, which predicts ICU mortality based on lab results and clinical data.[15] A pediatric version of the score has also received validation.[16]Septic Shock
In this scenario, which is associated with increased mortality, circulatory, and cellular/metabolic abnormalities such as serum lactate level greater than 2 mmol/L (18 mg/dL) are present. Because patients usually suffer from persisting hypotension despite volume resuscitation, the administration of vasopressors is required to maintain a mean arterial pressure (MAP) ≥ 65 mmHg.
Evaluation
Most countries are utilizing some type of clinical and epidemiologic information to determine who should have testing performed. In the United States, criteria have been developed for persons under investigation (PUI) for COVID-19. According to the U.S. CDC, most patients with confirmed COVID-19 have developed fever and/or symptoms of acute respiratory illness (e.g., cough, difficulty breathing). If a person is a PUI, it is recommended that practitioners immediately put in place infection control and prevention measures. Initially, they recommend testing for all other sources of respiratory infection. Additionally, they recommend using epidemiologic factors to assist in decision making. There are epidemiologic factors that assist in the decision on who test. This includes anyone who has had close contact with a patient with laboratory-confirmed COVID-19 within 14 days of symptom onset or a history of travel from affected geographic areas (presently China, Italy, Iran, Japan, and South Korea) within 14 days of symptom onset.
The WHO recommends collecting specimens from both the upper respiratory tract (naso- and oropharyngeal samples) and lower respiratory tract such as expectorated sputum, endotracheal aspirate, or bronchoalveolar lavage. The collection of BAL samples should only be performed in mechanically ventilated patients as lower respiratory tract samples seem to remain positive for a more extended period. The samples require storage at four degrees celsius. In the laboratory, amplification of the genetic material extracted from the saliva or mucus sample is through a reverse polymerase chain reaction (RT-PCR), which involves the synthesis of a double-stranded DNA molecule from an RNA mold. Once the genetic material is sufficient, the search is for those portions of the genetic code of the CoV that are conserved. The probes used are based on the initial gene sequence released by the Shanghai Public Health Clinical Center & School of Public Health, Fudan University, Shanghai, China on Virological.org, and subsequent confirmatory evaluation by additional labs. If the test result is positive, it is recommended that the test is repeated for verification. In patients with confirmed COVID-19 diagnosis, the laboratory evaluation should be repeated to evaluate for viral clearance prior to being released from observation.
The availability of testing will vary based on which country a person lives in with increasing availability occurring nearly daily.
Concerning laboratory examinations, in the early stage of the disease, a normal or decreased total white blood cell count and a decreased lymphocyte count can be demonstrated. Lymphopenia appears to be a negative prognostic factor. Increased values of liver enzymes, LDH, muscle enzymes, and C-reactive protein can be found. There is a normal procalcitonin value. In critical patients, D-dimer value is increased, blood lymphocytes decreased persistently, and laboratory alterations of multiorgan imbalance (high amylase, coagulation disorders, etc.) are found.
Treatment / Management
There is no specific antiviral treatment recommended for COVID-19, and no vaccine is currently available. The treatment is symptomatic, and oxygen therapy represents the major treatment intervention for patients with severe infection. Mechanical ventilation may be necessary in cases of respiratory failure refractory to oxygen therapy, whereas hemodynamic support is essential for managing septic shock.
On January 28, 2020, the WHO released a document summarizing WHO guidelines and scientific evidence derived from the treatment of previous epidemics from HCoVs. This document addresses measures for recognizing and sorting patients with severe acute respiratory disease; strategies for infection prevention and control; early supportive therapy and monitoring; a guideline for laboratory diagnosis; management of respiratory failure and ARDS; management of septic shock; prevention of complications; treatments; and considerations for pregnant patients.
Among these recommendations, we report the strategies for addressing respiratory failure, including protective mechanical ventilation and high-flow nasal oxygen (HFNO) or non-invasive ventilation (NIV).
Intubation and protective mechanical ventilation
Special precautions are necessary during intubation. The procedure should be executed by an expert operator who uses personal protective equipment (PPE) such as FFP3 or N95 mask, protective goggles, disposable gown long sleeve raincoat, disposable double socks, and gloves. If possible, rapid sequence intubation (RSI) should be performed. Preoxygenation (100% O2 for 5 minutes) should be performed via the continuous positive airway pressure (CPAP) method. Heat and moisture exchanger (HME) must be positioned between the mask and the circuit of the fan or between the mask and the ventilation balloon.
Mechanical ventilation should be with lower tidal volumes (4 to 6 ml/kg predicted body weight, PBW) and lower inspiratory pressures, reaching a plateau pressure (Pplat) < 28 to 30 cm H2O. PEEP must be as high as possible to maintain the driving pressure (Pplat-PEEP) as low as possible (< 14 cmH2O). Moreover, disconnections from the ventilator must be avoided for preventing loss of PEEP and atelectasis. Finally, the use of paralytics is not recommended unless PaO2/FiO2 < 150 mmHg. The prone ventilation for > 12 hours per day, and the use of a conservative fluid management strategy for ARDS patients without tissue hypoperfusion (strong recommendation) are emphasized.
Non-invasive ventilation
Concerning HFNO or non-invasive ventilation (NIV), the experts’ panel, points out that these approaches performed by systems with good interface fitting do not create widespread dispersion of exhaled air, and their use can be considered at low risk of airborne transmission.[17] Practically, non-invasive techniques can be used in non-severe forms of respiratory failure. However, if the scenario does not improve or even worsen within a short period of time (1–2 hours) the mechanical ventilation must be preferred.
Other therapies
Among other therapeutic strategies, systemic corticosteroids for the treatment of viral pneumonia or acute respiratory distress syndrome (ARDS) are not recommended. Moreover, unselective or inappropriate administration of antibiotics should be avoided. Although no antiviral treatments have been approved, alpha-interferon (e.g., 5 million units by aerosol inhalation twice per day), and lopinavir/ritonavir have been suggested. Preclinical studies suggested that remdesivir (GS5734) — an inhibitor of RNA polymerase with in vitro activity against multiple RNA viruses, including Ebola — could be effective for both prophylaxis and therapy of HCoVs infections.[18] This drug was positively tested in a rhesus macaque model of MERS-CoV infection.[19]
When the disease results in complex clinical pictures of MOD, organ function support in addition to respiratory support, is mandatory. Extracorporeal membrane oxygenation (ECMO) for patients with refractory hypoxemia despite lung-protective ventilation should merit consideration after a case-by-case analysis. It can be suggested for those with poor results to prone position ventilation.
Prevention
Preventive measures are the current strategy to limit the spread of cases. Because an epidemic will increase as long as R0 is greater than 1 (COVID-19 is 2.2), control measures must focus on reducing the value to less than 1.
Preventive strategies are focused on the isolation of patients and careful infection control, including appropriate measures to be adopted during the diagnosis and the provision of clinical care to an infected patient. For instance, droplet, contact, and airborne precautions should be adopted during specimen collection, and sputum induction should be avoided.
The WHO and other organizations have issued the following general recommendations:
-
Avoid close contact with subjects suffering from acute respiratory infections.
-
Wash your hands frequently, especially after contact with infected people or their environment.
-
Avoid unprotected contact with farm or wild animals.
-
People with symptoms of acute airway infection should keep their distance, cover coughs or sneezes with disposable tissues or clothes and wash their hands.
-
Strengthen, in particular, in emergency medicine departments, the application of strict hygiene measures for the prevention and control of infections.
-
Individuals that are immunocompromised should avoid public gatherings.
The most important strategy for the populous to undertake is to frequently wash their hands and use portable hand sanitizer and avoid contact with their face and mouth after interacting with a possibly contaminated environment.
Healthcare workers caring for infected individuals should utilize contact and airborne precautions to include PPE such as N95 or FFP3 masks, eye protection, gowns, and gloves to prevent transmission of the pathogen.
Meanwhile, scientific research is growing to develop a coronavirus vaccine. In recent days, China has announced the first animal tests, and researchers from the University of Queensland in Australia have also announced that, after completing the three-week in vitro study, they are moving on to animal testing. Furthermore, in the U.S., the National Institute for Allergy and Infectious Diseases (NIAID) has announced that a phase 1 trial has begun for a novel coronavirus immunization in Washington state.
Differential Diagnosis
The symptoms of the early stages of the disease are nonspecific. Differential diagnosis should include the possibility of a wide range of infectious and non-infectious (e.g., vasculitis, dermatomyositis) common respiratory disorders.
-
Adenovirus
-
Influenza
-
Human metapneumovirus (HmPV)
-
Parainfluenza
-
Respiratory syncytial virus (RSV)
-
Rhinovirus (common cold)
For suspected cases, rapid antigen detection, and other investigations should be adopted for evaluating common respiratory pathogens and non-infectious conditions.
Pertinent Studies and Ongoing Trials
Multiple studies globally are investigating the use of remdesivir, a broad-spectrum antiviral.
Prognosis
Preliminary data suggests the reported death rate ranges from 1% to 2% depending on the study and country. The majority of the fatalities have occurred in patients over 50 years of age. Young children appear to be mildly infected but may serve as a vector for additional transmission.
Complications
Long term complications among survivors of infection with SARS-CoV-2 having clinically significant COVID-19 disease are not yet available. The mortality rates for cases globally remain between 1% to 2%.
Deterrence and Patient Education
Patients and families should receive instruction to:
-
Avoid close contact with subjects suffering from acute respiratory infections.
-
Wash their hands frequently, especially after contact with sick people or their environment.
-
Avoid unprotected contact with farm or wild animals.
-
People with symptoms of acute airway infection should keep their distance, cover coughs or sneezes with disposable tissues or clothes and wash their hands.
-
Immunocompromised patients should avoid public exposure and public gatherings. If an immunocompromised individual must be in a closed space with multiple individuals present, such as a meeting in a small room; masks, gloves, and personal hygiene with antiseptic soap should be undertaken by those in close contact with the individual. In addition, prior room cleaning with antiseptic agents should be undertaken and performed before exposure. However, considering the danger involved to these individuals, exposure should be avoided unless a meeting, group event, etc. is a true emergency.
-
Strict personal hygiene measures are necessary for the prevention and control of this infection.
Enhancing Healthcare Team Outcomes
Since the first outbreak of coronavirus (COVID-19) in Wuhan, China, the disease is spreading worldwide. Individuals at the extreme of ages and those that are immunocompromised are at the most significant risk. All health care workers should understand the presentation of the disease, workup, and supportive care. Further, health professionals should be aware of the precautions necessary to avoid the contraction and spread of the disease. [Level 5]





References
- 1.
-
Perlman S, Netland J. Coronaviruses post-SARS: update on replication and pathogenesis.Nat. Rev. Microbiol. 2009 Jun;7(6):439-50.[PMC free article] [PubMed]
- 2.
-
Chan JF, To KK, Tse H, Jin DY, Yuen KY. Interspecies transmission and emergence of novel viruses: lessons from bats and birds.Trends Microbiol. 2013 Oct;21(10):544-55.[PubMed]
- 3.
-
Chen Y, Liu Q, Guo D. Emerging coronaviruses: Genome structure, replication, and pathogenesis.J. Med. Virol. 2020 Apr;92(4):418-423.[PubMed]
- 4.
-
Chan JF, Kok KH, Zhu Z, Chu H, To KK, Yuan S, Yuen KY. Genomic characterization of the 2019 novel human-pathogenic coronavirus isolated from a patient with atypical pneumonia after visiting Wuhan.Emerg Microbes Infect. 2020 Dec;9(1):221-236.[PubMed]
- 5.
-
Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, Ren R, Leung KSM, Lau EHY, Wong JY, Xing X, Xiang N, Wu Y, Li C, Chen Q, Li D, Liu T, Zhao J, Li M, Tu W, Chen C, Jin L, Yang R, Wang Q, Zhou S, Wang R, Liu H, Luo Y, Liu Y, Shao G, Li H, Tao Z, Yang Y, Deng Z, Liu B, Ma Z, Zhang Y, Shi G, Lam TTY, Wu JTK, Gao GF, Cowling BJ, Yang B, Leung GM, Feng Z. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia.N. Engl. J. Med. 2020 Jan 29;[PubMed]
- 6.
-
Bauch CT, Lloyd-Smith JO, Coffee MP, Galvani AP. Dynamically modeling SARS and other newly emerging respiratory illnesses: past, present, and future.Epidemiology. 2005 Nov;16(6):791-801.[PubMed]
- 7.
-
Lei J, Kusov Y, Hilgenfeld R. Nsp3 of coronaviruses: Structures and functions of a large multi-domain protein.Antiviral Res. 2018 Jan;149:58-74.[PubMed]
- 8.
-
Song W, Gui M, Wang X, Xiang Y. Cryo-EM structure of the SARS coronavirus spike glycoprotein in complex with its host cell receptor ACE2.PLoS Pathog. 2018 Aug;14(8):e1007236.[PubMed]
- 9.
-
Angeletti S, Benvenuto D, Bianchi M, Giovanetti M, Pascarella S, Ciccozzi M. COVID-2019: The role of the nsp2 and nsp3 in its pathogenesis.J. Med. Virol. 2020 Feb 21;[PubMed]
- 10.
-
Tian S, Hu W, Niu L, Liu H, Xu H, Xiao SY. Pulmonary pathology of early phase 2019 novel coronavirus (COVID-19) pneumonia in two patients with lung cancer.J Thorac Oncol. 2020 Feb 27;[PubMed]
- 11.
-
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H, Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China.Lancet. 2020 Feb 15;395(10223):497-506.[PubMed]
- 12.
-
Wu Z, McGoogan JM. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention.JAMA. 2020 Feb 24;[PubMed]
- 13.
-
Kogan A, Segel MJ, Ram E, Raanani E, Peled-Potashnik Y, Levin S, Sternik L. Acute Respiratory Distress Syndrome following Cardiac Surgery: Comparison of the American-European Consensus Conference Definition versus the Berlin Definition.Respiration. 2019;97(6):518-524.[PubMed]
- 14.
-
Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche JD, Coopersmith CM, Hotchkiss RS, Levy MM, Marshall JC, Martin GS, Opal SM, Rubenfeld GD, van der Poll T, Vincent JL, Angus DC. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3).JAMA. 2016 Feb 23;315(8):801-10.[PMC free article] [PubMed]
- 15.
-
Seymour CW, Kennedy JN, Wang S, Chang CH, Elliott CF, Xu Z, Berry S, Clermont G, Cooper G, Gomez H, Huang DT, Kellum JA, Mi Q, Opal SM, Talisa V, van der Poll T, Visweswaran S, Vodovotz Y, Weiss JC, Yealy DM, Yende S, Angus DC. Derivation, Validation, and Potential Treatment Implications of Novel Clinical Phenotypes for Sepsis.JAMA. 2019 May 28;321(20):2003-2017.[PubMed]
- 16.
-
Matics TJ, Sanchez-Pinto LN. Adaptation and Validation of a Pediatric Sequential Organ Failure Assessment Score and Evaluation of the Sepsis-3 Definitions in Critically Ill Children.JAMA Pediatr. 2017 Oct 02;171(10):e172352.[PMC free article] [PubMed]
- 17.
-
Hui DS, Chow BK, Lo T, Tsang OTY, Ko FW, Ng SS, Gin T, Chan MTV. Exhaled air dispersion during high-flow nasal cannula therapyversusCPAPviadifferent masks.Eur. Respir. J. 2019 Apr;53(4)[PubMed]
- 18.
-
Gordon CJ, Tchesnokov EP, Feng JY, Porter DP, Gotte M. The antiviral compound remdesivir potently inhibits RNA-dependent RNA polymerase from Middle East respiratory syndrome coronavirus.J. Biol. Chem. 2020 Feb 24;[PubMed]
- 19.
-
de Wit E, Feldmann F, Cronin J, Jordan R, Okumura A, Thomas T, Scott D, Cihlar T, Feldmann H. Prophylactic and therapeutic remdesivir (GS-5734) treatment in the rhesus macaque model of MERS-CoV infection.Proc. Natl. Acad. Sci. U.S.A. 2020 Feb 13;[PubMed]
Copyright© 2020, StatPearls Publishing LLC.
This book is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, a link is provided to the Creative Commons license, and any changes made are indicated.
In this Page
Similar articles in PubMed
- ReviewInsights into the Recent 2019 Novel Coronavirus (SARS-CoV-2) in Light of Past Human Coronavirus Outbreaks.[Pathogens. 2020]
- Novel coronavirus 2019-nCoV: prevalence, biological and clinical characteristics comparison with SARS-CoV and MERS-CoV.[Eur Rev Med Pharmacol Sci. 2020]
- ReviewSevere acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges.[Int J Antimicrob Agents. 2020]
- ReviewThe origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak – an update on the status.[Mil Med Res. 2020]
- Abelson Kinase Inhibitors Are Potent Inhibitors of Severe Acute Respiratory Syndrome Coronavirus and Middle East Respiratory Syndrome Coronavirus Fusion.[J Virol. 2016]
Recent Activity
Abstract
The severe acute respiratory syndrome (SARS)-coronavirus-2 (CoV-2) outbreak in Wuhan, China has now spread to many countries across the world including the UK with an increasing death toll. This will inevitably lead to an increase in the number of suspected coronavirus disease 2019 (COVID-19)-related deaths at autopsy. The Royal College of Pathologists has responded to this concern with the release of a briefing on autopsy practice relating to COVID-19. The following article is a summary and interpretation of these guidelines. It includes a description of hazard group 3 organisms, the category to which SARS-CoV-2 has been assigned, a brief description of what is currently known about the pathological and autopsy findings in COVID-19, a summary of the recommendations for conducting autopsies in suspected COVID-19 cases and the techniques for making the diagnosis at autopsy. It concludes by considering the clinicopathological correlation and notification of such cases.
Statistics from Altmetric.com
Introduction
The coronavirus family comprises several zoonotic viruses that cause serious human diseases including Middle East respiratory syndrome (MERS) and severe acute respiratory syndrome (SARS).1In late 2019, a new coronavirus outbreak due to SARS-coronavirus-2 (SARS-CoV-2) began in Wuhan, China, which causes an illness in humans designated as coronavirus disease 2019 (COVID-19) by the WHO.2COVID-19 pathobiology remains incompletely understood and significant efforts are underway to study it worldwide.
SARS-CoV-2 continues to spread as the number of deaths continue to increase.3The mode of transmission of the virus is thought to be largely by inhalation of respiratory droplets although acquisition via the skin surface is another possibility.4Fever is usually the first symptom with subsequent development of respiratory symptoms.5 6Most patients with COVID-19 have a mild disease course; however, approximately 20% develop severe disease with high mortality rate and is associated with older age and immunosuppression.5 6
In February 2020, the Royal College of Pathologists (RCPath) released guidance on postmortem examinations for mortuary workers in suspected COVID-19 cases.4This article summarises those guidelines. It is based on our current understanding of COVID-19 in early March 2020 and may change as more information becomes available.
Hazard group categorisation of COVID-19
In the UK, pathogens are categorised according to their risk to humans by the Advisory Committee on Dangerous Pathogens (ACDP) within the Health and Safety Executive.7ACDP guidance is largely aimed towards staff in clinical and research-related microbiology laboratories, however given the potential risk to the health of mortuary staff, autopsy practice has been adapted to reflect the risk of transmission of infectious pathogens during and after the postmortem examination.8These hazard groups (HG1–4) are assigned according to the risk of human infection, the likelihood spread and access to treatment or prophylaxis (seetable 1). Control of substances hazardous to health (COSHH) defines four containment levels for working with these, which correspond directly to the organism’s hazard group (ie, containment level 3 should be used for hazard group 3 organisms).
Table 1
ACDP hazard group definitions: table adapted from ref7
The SARS-related and MERS-related coronaviruses are both considered HG3 pathogens, while most otherCoronavirinaeare HG2.7SARS-CoV-2 has recently been categorised as a HG3 organism.4 7 9Other viruses within HG3 include rabies, poliovirus, dengue virus, hepatitis virus B, C, D and E, and HIV 1 and 2 among others.4Certain HG3 organisms (eg, hepatitis B, C, D and E virus) may be used at containment conditions less than those outlined by COSHH for HG3 organisms; however, SARS-CoV-2 is not on this list.7Once appropriate precautions are in place, the risk to mortuary workers dealing with these HG3 organisms are slight, and a well-staffed mortuary with experienced personnel should be capable of handling cases with any of these HG3 pathogens.
Risk reduction during postmortem examination in HG3 organisms
In general, conducting an autopsy on a patient with a suspected HG3 organisms requires four areas of attention: risk assessment, understanding of the pathology that may be found, universal standard precautions and any standard operating procedures for specific HG3 pathogens. The effective utilisation of universal precautions mitigates against inaccurate or incomplete information used in the risk assessment on an individual case basis.
Mortuary workers performing autopsies have a duty outlined by COSHH to perform risk assessments in every postmortem examination for the safety of themselves and their colleagues. Before the time of the autopsy, this may include a review of the clinical history on the consent form or coroner request form, information attained from the patient’s doctors, laboratory records and hospital infection control and external examination findings.
It must be stressed at this point that if the death is considered to be due to a confirmed COVID-19 infection, an autopsy is unlikely to be necessary and a Medical Certificate of Cause of Death should be given. However, if the infection is involved in a forensic case, then legal duty impels the proper performance of a full appropriate autopsy. The issue of whether a person dies with or from COVID-19 infection may not always be straightforward, and ongoing epidemiology and available investigation data may shed light on this.
Pathological findings in COVID-19
Information regarding the pathological findings in COVID-19 is limited, although several case reports have been published in recent weeks.10 11
Clinical features: Public Health England (PHE) has outlined criteria to assess possibility of COVID-19 infection in patients.12These criteria are the same when the patient is deceased with the exception that the timelines given in the guidance refer to the time prior death or onset of relevant symptoms before death where known.
If it is considered that COVID-19 may have been related to death by these criteria, the choice of either to perform a full postmortem or an examination is limited only to retrieving the samples required to verify COVID-19 infection. This decision must be made according to the individual case and should include the requirements of the coroner or any pertinent individuals. A staged postmortem may also be considered. This involves taking only diagnostic samples initially and later considering or a more complete autopsy after the results of these diagnostic tests are available. This staged technique is recommended if possible.
Macroscopic features: the macroscopic features of COVID-19 are likely to be in the chest and may include pleurisy, pericarditis, lung consolidation and pulmonary oedema. Lung weight may be increased above normal. It should be noted a secondary infection may be superimposed on the viral infection that can lead to purulent inflammation more typical of bacterial infection.4
Microscopic findings:a recent article described the early histopathological features in COVID-19 in two patients who underwent surgical resections for lung adenocarcinoma but were later discovered to have had COVID-19 at the time of the operation.11The findings were non-specific and included oedema, pneumocyte hyperplasia, focal inflammation and multinucleated giant cell formation while no hyaline membranes were seen. Given that these patients were asymptomatic with respect to COVID-19 at the time of the operation, these are likely to reflect only early changes of acute lung injury in the infection.11In another case, a 50-year-old man died from severe COVID-19 infection and more marked histopathological findings were noted.10Samples were taken by postmortem biopsy, and a description of the gross postmortem findings is not given, although multiple ground glass opacities were noted on chest X-ray. The microscopic findings included diffuse alveolar damage with exudates.10The inflammation was predominantly lymphocytic, and multinucleated giant cells were seen alongside large atypical pneumocytes, although no definitive viral inclusions were noted. Microvesicular steatosis with mild inflammation was noted in the liver, although it was unclear whether this was related to the virus or iatrogenic. The features are very similar to those seen in SARS and MERS-coronavirus infections.13 14
Mortuary factors
Adequate ventilation is need where HG3 autopsies are being performed with enough separation from the rest of the mortuary. Either whole room ventilation or down-drafts at the work stations are acceptable.15Any electric bone saws used should have a vacuum that isolates aerosolised particles. It is preferable to have an isolated high-risk facility for performing HG3 autopsies, although this is not compulsory.8All essential equipment should be brought at the start of the postmortem examination (eg, sample receptacles, culture bottles and so on) to eliminate the need to leave and re-enter the workspace. Further information may be found in the appropriate National Health Service guidance documents.16
The team available for these high-risk, postmortem examinations best includes the pathologist, the anatomic pathology technician (APT) and a third circulator. The presence of a circulator is beneficial but not essential.8Suitably experienced autopsy pathology trainees (as assessed by senior staff) may be involved in HG3 autopsies with adequate supervision. No specific infection risk to pregnant trainees has been identified; however, they may decide not to undertake autopsy work, and this should be discussed with the deanery.
Performance of the autopsy in HG3 infections
Several techniques undertaken at autopsy can reduce the risks encountered by HG3 infections. Personnel must be adequately trained. For APTs, this exposure should be in line with their curriculum and standardised training under the Royal Society for Public Health. For pathology trainees, this is at the discretion of senior staff. Sharps injuries can be reduced by minimising sharps in the workspace, using round-ended scissors, blunt-ended PM40 blades and having only a single operator working in the body cavity at a time.4Fresh organs should be sliced while being stabilised with a sponge on a solid surface. Needles should be placed in sharps bins and never resheathed.
Personal protective equipment (PPE) is vital. Certain PPE is universally used in postmortem examinations (box 1); however, the typical surgical masks are not considered sufficient protection. Valved fold flat and moulded protection masks are over 95% effective and are suitable for use in anticipated COVID-19 cases.4Whole-body suits with individual respirators seem to provide almost complete protection, although these are impractical and not necessary.15
Box 1
List of minimum personal protective equipment (PPE) in suspected coronavirus disease 2019 (COVID-19) cases
Universal PPE
-
Surgical scrubs.
-
Scrub hat.
-
Clear face visor.
-
Waterproof gown to cover whole body and forearms (typically a surgical gown).
-
Plastic apron.
-
Rubber boots with metal toecaps.
-
Protective kevlar or neoprene cut-resistant under-gloves.
-
Single use disposable non-latex gloves.
Additional protective equipment in suspected COVID-19 cases
-
Fold flat and moulded protection mask or whole-body suit.
A staged postmortem is recommended by RCPath.4Where a more detailed examination is necessary, a limited postmortem may be considered. In widespread infections, a minimally invasive postmortem examination can be performed to provide necessary fluid and tissue samples;17however, regional or localised infections may be difficult to identify with this technique alone, although they may be improved by combination with postmortem imaging.
Postmortem CT (PMCT) examination:histopathologists with local agreements regarding access to scanning facilities may contemplate PMCT to demonstrate significant pulmonary findings or identify causes of death in a case with incidental SARS-CoV-2 infection. A recently multicentre study (n=101) showed ground-glass lung opacities in 86% of cases, or mixed ground-glass and consolidation in 64% of patients examined.18Vascular enlargement and traction bronchiectasis are also described (71% and 53%, respectively). The changes were more likely to be bilateral, peripherally distributed and involving the lower lobes. The decision to undertake native PMCT or ventilated PMCT would be for the reporting radiologist following consultation: use of an existing clinical airway, or creation of a tracheostomy postmortem, would provide access for ventilation and potentially lower respiratory tract sampling.
Diagnosis of COVID-19
The samples required to diagnose COVID-19 at autopsy are the same as those required during life. They include a 5 mL sample of plain blood (no additive) for serology, upper aerodigestive tract swabs (nose and throat) and lower respiratory tract samples (bronchoalveolar lavage or sputum).19For full and up-to-date details on how to submit these samples, one should follow the links in the references.19It should be noted that the submission of each sample requires a specific E28 form. The specific advice from PHE is that one swab should be used for the upper aerodigestive tract and another swab for the lower respiratory tract.4
RCPath recommends that standard samples, such as respiratory tract swabs and tissue samples, should also be sent to local microbiology departments simultaneously to detect pathogens in the differential diagnosis. Where possible, a complete set of tissue histology is also recommended along with other specific investigations as outlined on a case-by-case basis. Standard formalin-fixation inactivates known coronaviruses and SARS-CoV-2 is believed to be similarly affected.20
Ready-to-use swabs can collect respiratory tract samples. Blood, urine and cerebrospinal fluid samples, where deemed appropriate, should be taken prior to opening the body cavity and under as sterile conditions as possible to reduce contamination. This may be achieved using alcohol-containing disinfectant to clean the skin. Blood cultures should be taken preferentially from the subclavian vein, jugular vein or left ventricle to reduce contamination from the bowel.
Conclusion
We have outlined the hazard group categorisation, pathological features and approach to the autopsy in suspected COVID-19 cases to aid mortuary workers. If on clinicopathological correlation, COVID-19 is deemed to be primary cause of death, then it should be given at the last line of part 1 in the Office of National Statistics format. If there is another primary cause of death and COVID-19 is considered to be contributory, then it can be put in part 2. Finally, it is worthwhile to notify PHE of any cases where COVID-19 is confirmed, although this should also be done by the laboratory that made the diagnosis.
References
Footnotes
-
Handling editorTahir S Pillay.
-
Correction noticeThis article has been corrected since it appeared Online First. The abstract has been replaced, and a new sentence and reference added “Standard formalin-fixation inactivates known coronaviruses and SARS-CoV-2 is believed to be similarly affected[20]”. Several minor text changes have been made throughout.
-
ContributorsBH designed and planned the manuscript performed the literature review, wrote the paper and collaborated with other authors in review. SBL, EY and BS reviewed manuscript drafts and contributed several paragraphs. MO designed and planned the manuscript and was involved in review of drafts along with collaborating between coauthors for multidisciplinary input.
-
FundingThe authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interestsNone declared.
-
Patient consent for publicationNot required.
-
Provenance and peer reviewCommissioned; internally peer reviewed.
Request Permissions
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
Copyright information:
FIGURE 1.
Computed tomographic images obtained from the patient 3 weeks after initial clinical manifestations of COVID-19 and 2 weeks before transthoracic biopsy, demonstrating ground glass–like opacifications.
Pleural thickening and enlarged mediastinal lymph nodes were present. Arrows indicate the approximate locations of the subsequently obtained postmortem transthoracic needle biopsy samples. A. Left upper anterior segment. B. Left upper lingular segment. C. Left lower lobe.

FIGURE 1.
Continued

FIGURE 2.
Histopathologic examination of lung biopsy tissues and immunostaining from a patient who died of COVID-19 (×100 magnification).
A. Histopathologic examination revealing diffuse alveolar damage, organizing phase (A-1); denudation of alveolar lining cells (arrow 1), with presence of reactive type II pneumocyte hyperplasia (arrow 2) (A-2); intra-alveolar fibrinous exudates (arrow 3) and interstitial loose fibrosis with chronic inflammatory infiltrates (arrow 4) (A-3); and intra-alveolar loose fibrous plugs (arrow 5) (A-4). In most foci, intra-alveolar organizing fibrin is seen (arrow 6). B. Immunostaining of SARS-CoV-2 in lung sections. Images were taken under light and fluorescent conditions, respectively (×100 magnification). Merged images were also generated. Blue arrows indicate interstitial areas between the alveoli, and green arrows indicate injured epithelial cells desquamated into the alveolar spaces. The dashed black lines indicate the blood vessel. Immunostaining of SARS-CoV-2 was done by using a rabbit polyclonal antibody (made in house, 1:100) against the Rp3 NP protein, which is highly conserved between SARS-CoV and SARS-CoV-2, followed by probing with a Cy3-conjugated goat antirabbit IgG (1:50, Abcam, ab6939). C. Positive and negative controls for immunostaining. For the positive control, the Huh7 cells were infected with SARS-CoV-2 at multiplicity of infection of 0.5 for 48 hours. After extensive washes, the cells were then fixed with 2.5% (wt/vol) glutaraldehyde. The infected cells were stained in red, and nuclei were stained with DAPI (Beyotime, Wuhan, China) in blue. For the negative control, biopsy lung sections derived from a patient with HIV who died of fungal infection were stained in parallel with lung sections from the patient with COVID-19 as above.

References
-
ZhouP
,
YangXL,
WangXG,
et alA pneumonia outbreak associated with a new coronavirus of probable bat origin.Nature2020 -
CormanVM
,
LandtO,
KaiserM,
et alDetection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR.Euro Surveill202025